
 A world without breasts.
A world without breasts.
We are mammals. We belong to a class of animals that feed their young by producing milk in specialized glands. These glands are so important, that they have enabled our species to flourish and evolve. It allows our offspring to take their time developing until they can chew and eat unassisted. Sounds pretty important right? So imagine if you will, the proposition that circumcising a baby boy to prevent potential adverse health outcomes later in life would be just like “chopping off” breast buds to prevent breast cancer. I have heard this argument from anti-circumcision proponents (intactivists) so many times I can go into any thread about infant circumcision (or female genital mutilation, which is always redirected to male circumcision) and go to the comments and count down 3..2..1. boom, there it goes. “Guys! I guess we should cut off all breast buds to prevent 100% of breast cancer in women!! Makes sense!” The problem with this trope is that the people who keep repeating it have not thought it through for more than 3 seconds. I am going to specifically talk about prophylactic mastectomy because it’s the most complex, but intactivists will insert a random body part into this argument all the time, i.e. tonsils, appendix, etc. Many of the following arguments also apply to surgeries such as appendectomy and tonsillectomy, but for slightly different reasons.

Breast buds are not present at birth. A lesson in human development.
Let’s start with basic anatomy and human development, intactabuddies. Breast buds are one of the first signs of female puberty, also known as thelarche, that typically begins in girls between 8 and 13 years old. Baby boys and girls’ breast tissue are nearly identical at birth, down to the nipples and milk ducts, until puberty when a magical thing happens when female hormones from the ovaries, mainly estrogen, acts upon the breast tissue to start forming breast buds. Males secrete testosterone, and this helps to block breast formation. If you were the surgeon tasked with removing breast buds, what is the difference in which tissue you would be removing from the newborn girl vs. baby boy? That’s a trick question, because newborns don’t have breast buds! There are some cases where newborn boys or girls can be born with breast buds from a burst of estrogen received from the mother, but they resolve over 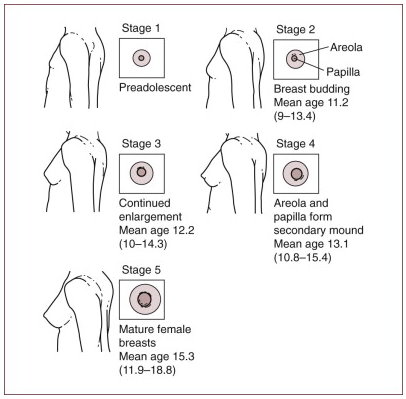 time. That means you would not be able to perform this surgery on newborns, you would have to at least wait until puberty. If you were to round up a few million 8-13 year old girls and surgically remove all their breast buds, you could indeed drastically reduce breast cancer, in a world without breasts. If you didn’t care about their band practice, science club, their Frozen themed birthday parties or their gymnastics practices, and pulling them out of school and painfully out of commission for at least 4-6 weeks, sure. This is the first of many differences of from routine infant circumcision, you would need to perform the prophylactic surgeries on young girls, not newborns. Their own logic prevents this scenario anyway as they believe that no minor should have any alteration to their bodies as they can’t give consent, leaving only prophylactic mastectomy on adults with fully formed breasts.
time. That means you would not be able to perform this surgery on newborns, you would have to at least wait until puberty. If you were to round up a few million 8-13 year old girls and surgically remove all their breast buds, you could indeed drastically reduce breast cancer, in a world without breasts. If you didn’t care about their band practice, science club, their Frozen themed birthday parties or their gymnastics practices, and pulling them out of school and painfully out of commission for at least 4-6 weeks, sure. This is the first of many differences of from routine infant circumcision, you would need to perform the prophylactic surgeries on young girls, not newborns. Their own logic prevents this scenario anyway as they believe that no minor should have any alteration to their bodies as they can’t give consent, leaving only prophylactic mastectomy on adults with fully formed breasts.
If Angelina Jolie were dead, she would be rolling in her grave.
Let’s talk about how and why prophylactic mastectomies(PM) are currently performed in women and what their benefits and risks are. First of all, you may have noticed I said we could “reduce” breast cancer risk, but I did not say we could eliminate it. If you surgically remove breast tissue, how can you still get breast cancer? The Mayo Clinic explains, “Having a prophylactic mastectomy doesn’t guarantee that you’ll never develop breast cancer because all of your breast tissue can’t be removed during the surgery. Sometimes breast tissue can be found in your chest, armpit or skin, above your collarbone, or on the upper part of your abdominal wall.” Currently the only females that doctors recommend undergo prophylactic mastectomy are:
- Already had cancer in one breast.
- A strong family history of breast cancer.
- Positive results from gene testing such as BRCA1 and BRCA2 mutations.
- Breast changes that significantly increase your risk of cancer such as lobular carcinoma in situ (LCIS).
- Radiation therapy to the chest area at a young age.
- Dense breasts, especially accompanied by other high risk factors.
In female patients with BRCA1 and BRCA2 mutations, “prophylactic mastectomy reduces the risk of developing breast cancer by up to 90 percent.” This means that even if you removed breast buds from every girl on the planet, females with the BRCA mutations still have a 10% chance of developing breast cancer.
The above recommendations are for adult women who undergo mastectomy of fully developed breasts, not children with breast buds. This makes it difficult to assess the actual risks of breast bud removal because it simply isn’t done. In fact, a true prophylactic breast bud removal is extremely rare and considered highly unethical. We can point to the case precedent of Ashley X, a 9 year old girl with static encephalopathy who in a national spotlight underwent a very controversial “growth attenuation” therapy with high dose estrogen to essentially freeze her in her child-like form forever so her parents could more easily take care of her. The child’s uterus and breast buds were illegally surgically removed without obtaining a court order to protect against developing an estrogen mediated breast cancer, as well as preventing menstruation. However, as with all parents, they were making medical decisions for their child since all children are unable to consent. All medical care isn’t just acute treatments, some care is preventative, such as vaccinations. Vaccinating carries some risk, albeit very small but the overwhelming benefits of vaccinating greatly outnumber the risks. The risks espoused by antivaxxers are also misunderstood, exaggerated or simply not true. The world’s scientific community has a consensus in favor of the overall safety and benefits of vaccinations. It is quite telling that many intactivists are also antivaxxers. They simply don’t understand the scientific literature and their main goal is to push an agenda at all costs, even if it means lying or hurting children. So how do parents, in conjunction with their doctors, make decisions for their children’s health? They weigh the benefits vs. risks, and decided what is important to them.
Breasts and foreskins aren’t the same.
I can hear the intactivists now. “It was illegal for the doctors to perform hysterectomy and breast bud removal on Ashley X, therefore it is just as unethical to remove the foreskin from boys!” I understand that intactivists aren’t really advocating for breast bud removal when they make their silly argument, rather they are making a flippant assertion that a foreskin=breasts, and therefore the removal of either is just as unethical. This is not true when you look at the function of each, and what risks there are in removing them when weighed with the benefits. The concept of benefits vs. risks is lost on most intactivists, and many times the risks are severely distorted and the benefits are swept under the rug. So let’s make a comparison of the risks vs benefits of RIC vs PM. One thing to consider before we lay out the risks/benefit analysis is that this has already been done by the premier authority on the health and welfare of children in this country, the American Academy of Pediatrics. “The AAP is a professional membership organization of 62,000 primary care pediatricians, pediatric medical sub-specialists and pediatric surgical specialists dedicated to the health, safety, and well being of infants, children, adolescents and young adults.” The AAP has performed a systematic review of ALL available current scientific literature, which is simply the best form of scientific evidence available.  These aren’t layperson self appointed keyboard warriors with personal opinions and a poor grasp of scientific literature, these are professionals, doctors, PhDs, mothers and fathers with children of their own. They have the benefit of seeing the big picture, having access to all of the up to date, non biased medical information. If a newborn died from the complications of circumcision, they would be the ones who see it. So what does the AAP say after performing their exhaustive systematic review?
These aren’t layperson self appointed keyboard warriors with personal opinions and a poor grasp of scientific literature, these are professionals, doctors, PhDs, mothers and fathers with children of their own. They have the benefit of seeing the big picture, having access to all of the up to date, non biased medical information. If a newborn died from the complications of circumcision, they would be the ones who see it. So what does the AAP say after performing their exhaustive systematic review?
The AAP statement on newborn male circumcision says “that preventive health benefits of elective circumcision of male newborns outweigh the risks of the procedure. Benefits include significant reductions in the risk of urinary tract infection in the first year of life and, subsequently, in the risk of heterosexual acquisition of HIV and the transmission of other sexually transmitted infections.
The procedure is well tolerated when performed by trained professionals under sterile conditions with appropriate pain management. Complications are infrequent; most are minor, and severe complications are rare. Male circumcision performed during the newborn period has considerably lower complication rates than when performed later in life.”
The risks associated with prophylactic mastectomy, however are significantly more serious, and according to breastcancer.org are as follows:
Risks immediately after surgery:
- bleeding or infection
- fluid collecting under the scar
- delayed wound healing
- scar tissue formation
Long-term risks:
- Prophylactic mastectomy is permanent and irreversible.
- This surgery causes significant loss of sensation in the breast, which can have an impact on sexuality.
- Women who undergo prophylactic mastectomy will no longer have the ability to breastfeed from the affected breast(s).
- After prophylactic mastectomy, some women experience anxiety or depression about body image.
In addition to these risks, there have been some alarming data that postmastectomy pain syndrome is seen in about 23.9% of women who have undergone the surgery. The long term risks are psychologically and emotionally damaging to many women as it robs them of feeling feminine, along with a tremendous sense of loss and guilt with not being able to breastfeed.
In contrast the risks of RIC are as follows:
“Two large US hospital-based studies with good evidence estimate the risk of significant acute circumcision complications in the United States to be between 0.19% and 0.22%.121,123 Bleeding was the most common complication (0.08% to 0.18%), followed by infection (0.06%) and penile injury (0.04%). For comparison, an audit of 33,921 tonsillectomies found an incidence of hemorrhage of 1.9% among children aged 0 to 4 years.” Furthermore, bleeding from a tonsillectomy is not the same as bleeding from a penis. A parent can be instructed to hold pressure on a bleeding foreskin, this can’t be done inside the mouth by a parent. Holding pressure stops bleeding virtually 100% of the time. In addition to not being able to hold pressure in a post tonsillectomy bleed, bleeding into an already swollen airway can be catastrophic. All bleeding isn’t the same. Many times, intactivists with their poor understanding of medicine will incorrectly equate the above scenarios, when in reality they are nothing alike. Again, it’s weighing benefits vs. risks. An interesting thing happens in surgery when risks and benefits of two different things converge. For example, when a bowel surgery is necessary such as a colectomy (removal of colon) or cystectomy (removal of bladder), surgeons will often perform an appendectomy even if the patient doesn’t have acute appendicitis. Why? The patient has already incurred the risks of an intraabdominal surgery, aka bleeding, infection, organ damage, so the added benefit of preventing acute appendicitis in the future is gained without added risk. This is why preventative appendectomies aren’t performed, because by itself the risk of intraabdominal surgery is much, much greater than the benefits.
There are late complications of newborn circumcision that can also occur, although uncommon and include “excessive residual skin (incomplete circumcision), excessive skin removal, adhesions (natural and vascularized skin bridges), meatal stenosis, phimosis, and epithelial inclusion cysts. These complications are considered “late,” as opposed to “acute” (or immediate) complications such as bleeding or infection, which may still present during infancy but not during the immediate postprocedural time frame.” Meatal stenosis has been shown to be 100% preventable by applying petroleum jelly to the tip of the penis post circumcision. This is because the circumcision is not the cause of the stenosis, only a risk factor. The causative agent is the inflammation of the meatus in a urine soaked diaper, so petroleum jelly provides a barrier to the urine.
Classic false equivalency
Intactivists love to invoke logical fallacies in their arguments. A false equivalency is when two things are compared that seem similar but are totally different. This can be illustrated when you actually go through with the above scenario and actually circumcise all boys and perform PM on all females. What would those two scenarios look like? First, imagine a world that all males have their foreskins circumcised within 1 month of birth with a couple milliliters of lidocaine (local anesthesia). They have a few days of healing with minor discomfort, without a single suture. The males, as a result, don’t have a mucosal fold of skin on the tip on their penis for the rest of their lives. Sounds like a nightmare, right? This is a world in which males still experience the joys of masturbating, sexual ecstasy of penile in vagina, in anal and in oral intercourse. They can have children, have successful careers, a wonderful fulfilling relationship and have the potential to live life to the fullest.
Now imagine the other scenario in which every 8-13 year old girl is taken out of commission for 4-6 weeks to perform mastectomies on their breast buds, and in effect eliminating breasts from this planet henceforth. I mean, it’s not like breasts are part of a women’s femininity, sexuality or used to feed the entirety of humanity and the basis for an entire class of animals called MAMMals, right? Infant formula is a modern invention which has drastically improved infant mortality rates in developed worlds. It allows for infants to survive in situations where the mother dies or is not able to effectively breast feed. We would be extinct as a species if PM were performed on every female. Lack of foreskin? Still able to reproduce and feed young all the while reducing some disease. Do you see how the two are not even remotely comparable? Do you see how one is not like the other? Do you see how the risks and benefits are not even in the same ballpark? Stop using this argument, Intactivists. It exposes how woefully misinformed you are on biology, how you are incapable of understanding risk/benefit ratios and how dismissive you are of evidence.

Speaking of fallacy; your assertion that, because puberty initiates breast tissue differentiation, an intactivist’s comparison to RIC must be to a pubescent girl is a strawman. Infant breast tissue could be easily removed surgically without waiting for puberty to effect a reduction in breast cancer in BRCA-mutants and, when performed by trained professionals under sterile conditions with appropriate pain management, would likely have similar healing times as RIC with fewer complications (less local exposure to pathogens). I appreciate your approach to the argument, but your strawman makes this piece hypocritical.
LikeLiked by 1 person
The article clearly stated that breast buds are not present in most newborn baby girls (or boys for that matter). So, excising breast buds in the neonatal period is not possible. At birth, the chest wall is surmounted with the pectoral muscles. When a woman has a breast removal surgery (due to cancer or whatever) the surgeon sometimes removes all or part of the pectoral muscle. This is a severe complication to the health and physical capability of the woman. In the neonate, such reduction surgery would be disabling. And, the recovery period would be protracted, not days as in MIC and offer the opportunity for far more and severe after effects.
Not a fallacy or strawman at all.
LikeLike
You went through a lot of trouble to avoid the baseline analogy of informed consent. You’re also a misandrist bigot who has no respect for male bodily autonomy, and is involved in body shaming the natural male body. Finally, you’re an uneducated dunce in the facts (facts as in, non-negotiable medical science) of the foreskin. This was like reading the death throes of a sad, mentally ill and sick ideology of female superiority. You’re a disgrace to human beings.
LikeLiked by 1 person
Sounds like a lot of projection. You really should seek mental hello sir.
LikeLiked by 1 person
The infant cannot give informed consent. For this they depend on their parents or legal guardians operating under the advice and guidance of appropriate health care professionals.
This is well understood, being in UN articles signed by most of the world nations, legal and ethical society articles, AMA, AAP, WHO, the common law of most nations and multiple supporting court decisions that, in summary, give wide latitude to the parents to make decisions for the child that they believe will be of benefit to the child either currently or in the future.
Bodily autonomy is also not absolute, either for the infant of the adult. This is also covered by the above mentioned sources.
Also, the foreskin exists in a range of configurations from non-existent to extending far past the glans. Babies are born without a foreskin (Mohammed, the current Israeli premier).
http://www.aboutcirc.com/skintype.htm
http://www.male-initiation.net/library/medicus/schoeberlein_eng.html
And, finally, most sites on which I post attempt to have a civil discourse. Quora, for instance, has the stated policy of BNBR for Be Nice, Be Respectful. On other sites, the moderator deletes such posts as yours. The English language is very expressive, and civilized exposition can convey your meaning without inflammatory rhetoric.
LikeLike